

Federal Regulatory and Reimbursement Changes - Telehealth and Covid-19
This information is prepared for informational purposes only, and should not be considered legal advice. For more complete and up-to-date advice, please consult with your attorney and/or Primary Care Association.
Information is up to date as of May 1, 2023.
Medicare Telehealth Billing Guidelines for FQHCs during and after the Covid-19 Public Health Emergency
Guidelines, regulations, terms, and definitions mentioned here are specific to Medicare Telemedicine, Telehealth, and other forms of Virtual Communications for FQHCs during and after the Covid-19 pandemic. Please check back for updates and direct all questions or concerns to support@healthefficient.org.
On January 30, 2023, The Biden Administration announced its intent to end the Covid-19 public health emergency (PHE) declarations on May 11, 2023. The Consolidated Appropriations Act, 2023 (CAA, 2023) includes a provision that extends certain flexibilities in place during the PHE through December 31, 2024, including allowing FQHCs to furnish telehealth services as distant site providers. The CAA, 2023 also delays the in-person requirements for mental health visits via telecommunications technology until January 1, 2025.
CMS has developed a Coronavirus waivers & flexibilities webpage which contains details on all waivers and includes new provider-specific fact sheets. These fact sheets detail the phased “cross-cutting initiative” CMS has developed to evaluate CMS-issued PHE waivers and flexibilities to prepare the health care system for operation after the PHE.
Contents
Provider Enrollment and Licensing
During the PHE, CMS expedited any pending or new applications from providers and suppliers, including physicians and non-physician practitioners, received on or after March 1, 2020. When the PHE ends, CMS will resume normal application processing times. Toll-free enrollment hotlines that were established during the PHE will be shut down on May 11, 2023. Providers can find general support with telehealth licensure on the HHS Telehealth website.
Points of Clarification
Cost-sharing
For service dates beginning March 18, 2020, and through the duration of the PHE, CMS will pay all of the reasonable costs for specified categories of E/M services if they result in an order for or administration of a Covid-19 test, relate to the furnishing or administration of such test OR to the evaluation of a beneficiary for purposes of determining the need for such test. For such services, including when furnished via telehealth, RHCs and FQHCs must waive the beneficiary’s coinsurance. Applicable claims should be submitted with modifier CS appended to the appropriate service line. The Office of Inspector General issued a Policy Statement to notify physicians and other practitioners that they will not be subject to administrative sanctions for reducing or waiving any cost-sharing obligations Federal health care program beneficiaries may owe for telehealth services furnished during the PHE.
Patient Consent
Per CMS, the patient must give verbal consent for each telehealth encounter and documented in the medical record. CMS has stated it is acceptable to obtain this consent at the same time the services are initially furnished and for care management and virtual check-ins, annual informed consent will suffice. However, it is best practice to obtain consent for each encounter to err on the side of caution and minimize confusion for providers. Beneficiary consent to receive these services may be obtained by auxiliary personnel under general supervision of the RHC or FQHC practitioner; and the person obtaining consent can be an employee, independent contractor, or leased employee of the RHC or FQHC practitioner. If your state has different requirements, then the most stringent guidelines should be applied.
The following information must be communicated to the patient as part of consent:
Virtual visits are not being recorded
Establish a method to resume a dropped/disconnected visit whether it be reconnecting or having the patient dial a specific number
Confidentiality risks whenever applicable
Emergency procedures and local emergency departments
Exhibit virtual etiquette (connect from a quiet, private, safe environment with minimal distractions)
Medical record documentation, regardless of visit type
Patient consent
Location of patient
Location of provider
Note the services were rendered virtually, mentioning the mode of technology used
Names of any additional providers or other professionals consulting or assisting the patient
Any difficulty using equipment that impacts the time or quality of the visit
Lack of adequate connectivity or secure environment
Inability to collect necessary medical information necessary to perform an adequate exam
Telehealth Visits
Telehealth allows certain provider types to furnish services that would generally occur in-person via interactive telecommunications systems, defined by CMS as multimedia communications equipment that includes, at minimum, audio and video equipment permitting two-way, real-time interactive communication between the patient and distant site physician or practitioner.
In 2022 CMS amended the definition of interactive telecommunications systems to include audio-only when used for telehealth services for the diagnosis, evaluation or treatment of mental health disorders furnished to established patients in their homes under certain circumstances.
Additionally, the definition of an FQHC Mental Health Visit was also amended to include interactive telecommunications technologies. Audio-only will be permitted when the patient is not capable of or does not consent to the use of video. Both amendments carry the condition that the patient must be seen in-person within six months prior to the initial telehealth encounter and subsequently every 12 months. FQHCs will be reimbursed their PPS rate for these visits with the appropriate modifier indicating the type of technology. The in-person requirements for these visits are currently waived through December 31, 2024.
Store-and-forward technologies are billable by FQHCs only when furnished in Alaska or Hawaii, under specific circumstances.
Eligible Provider Types
The FQHC clinician must be an enrolled Medicare “core practitioner”:
Physician
Nurse Practitioner (NP)
Physician Assistant (PA)
Certified Nurse Midwife (CNM)
Clinical Psychologist (CP)
Licensed Clinical Social Worker (LCSW)
Originating Sites (location of patient/beneficiary)
Geographic and site limitations for originating sites have been temporarily removed for the duration of the Covid-19 public health emergency, allowing the patient’s home to be an acceptable originating site. The 2022 PFS final rule allows the patient home as an originating site for mental health services under the aforementioned conditions.
Distant Sites (location of provider)
FQHCs and RHCs can be distant site providers during the Covid-19 pandemic only. FQHC/RHC providers may provide telehealth services from any location, including their home, during the facility’s usual working hours. This waiver is currently applicable through December 31, 2024.
Coding Covered Services
Medicare providers should be coding their charts according to the services rendered. Under the Section 1135 waiver expansion of telehealth services, Medicare beneficiaries can receive evaluation and management (E&M) visits, mental health counseling and preventive health screenings via telehealth, regardless of the patient’s diagnosis.
Temporary additions to telehealth covered services include audio only CPTs 99441-99443 which are not limited by provider type for the duration of the public health emergency, taking into consideration the CPT code description for the services. The following link will provide all covered CPTs including temporarily covered services which are denoted separately: List of Telehealth Services Payable Under the Medicare Physician Fee Schedule
Billing – FQHC Originating Site
Claim type: UB-04 billed to Part A
Do not append PPS code
HCPCS Q3014, Revenue code 0780
Type of Bill (TOB) 771 FQHC
Billing – FQHC Distant Site
Claim type: UB-04 billed to Part A
Do not append PPS code
HCPCS G2025, revenue code 0521
Type of Bill (TOB) 771 FQHC
Reimbursement
FQHCs that serve as originating sites for telehealth services get an originating site facility fee. Although FQHC services billed to Part B are not traditionally subject to deductible, the facility fee is not considered an FQHC service and therefore the deductible must be applied. The 2022 fee for Q3014 was set at $27.59, currently set at $28.64 for 2023.
FQHC distant site claims billed via G2025 are reimbursed $95.88 effective January 1, 2023. The 2022 reimbursement rate was $97.24. MACs will automatically reprocess claims that may have been reimbursed at the old rate before the adjudication system was updated.
*Mental health services rendered by FQHCs via telecommunications systems are not considered telehealth and are eligible to be billed and reimbursed via PPS code with the proper modifier appended to indicate modality. Please see the Billing Matrix at the end of this page for more information.
Virtual Communication Services
Virtual Check-ins
These are brief virtual encounters where a provider gives the patient at least 5 minutes of a billable FQHC communication technology-based or remote evaluation service. There are no geographic limitations or restrictions on providers or patients, meaning home/residence is an acceptable location for both parties. These are not considered telehealth, but consent must still be obtained.
General Requirements
Visit must be initiated by the patient
Patient did not get any FQHC-related service within the previous 7 days or the virtual encounter or remote evaluation AND does not need an FQHC service within the next 24 hours or, at the soonest available appointment
If the visit is related to an FQHC encounter that occurred in the last 7 days, the virtual encounter will be considered bundled to the prior visit
If the visit leads to a subsequent encounter within the next 24 hours or soonest available appointment, the subsequent visit will be considered bundled to the virtual encounter
Technology
Audio-video
Audio-only
Secure email or text
EHR/Patient Portal
Coding
G0071: Payment for communication technology-based services for 5 minutes or more of a virtual (non-face-to-face) communication between an rural health clinic (RHC) or federally qualified health center (FQHC) practitioner and RHC or FQHC patient, or 5 minutes or more of remote evaluation of recorded video and/or images by an RHC or FQHC practitioner, occurring in lieu of an office visit; RHC or FQHC only
The following HCPCS code is represented by G0071 for virtual check-ins and do not need to be appended separately. The medical record should be documented accordingly:
G2012: Brief communication technology-based service, e.g. virtual check-in, by a physician or other qualified health care professional who can report evaluation and management services, provided to an established patient, not originating from a related e/m service provided within the previous 7 days nor leading to an e/m service or procedure within the next 24 hours or soonest available appointment; 5-10 minutes of medical discussion
Billing
Claim Type: UB-04 billed to Part A
Do not append PPS code
HCPCS G0071, revenue code 0521
Type of Bill (TOB) 771 for FQHC
E-Visits
E-visits are digital assessments where the provider spends at least 5 minutes or more over the course of seven days providing online E&M services. Allowed in all types of locations, including the patient’s home, with no geographic limitations.
General Requirements
Patient must initiate the encounter
Communications occur over a 7-day period
Cumulative; for another 7-day period to begin, the patient must initiate a new communication through the portal. Documentation must justify the amount of time spent
Technology
Secure email or text
EHR/Patient Portal
Coding
G0071: Payment for communication technology-based services for 5 minutes or more of a virtual (non-face-to-face) communication between an rural health clinic (RHC) or federally qualified health center (FQHC) practitioner and RHC or FQHC patient, or 5 minutes or more of remote evaluation of recorded video and/or images by an RHC or FQHC practitioner, occurring in lieu of an office visit; RHC or FQHC only
The following CPTs are represented by G0071 for virtual check-ins and do not need to be appended separately. The medical record should be documented accordingly:
99421: Online digital evaluation and management service, for an established patient, for up to 7 days, cumulative time during the 7 days; 5–10 minutes
99422: Online digital evaluation and management service, for an established patient, for up to 7 days cumulative time during the 7 days; 11– 20 minutes
99423: Online digital evaluation and management service, for an established patient, for up to 7 days, cumulative time during the 7 days; 21 or more minutes
Billing
Claim Type: UB-04 billed to Part A
Do not append PPS code
HCPCS G0071, revenue code 0521
Type of Bill (TOB) 771 for FQHC
Reimbursement – G0071 (Virtual Check-ins and E-Visits)
Medicare will not reimburse FQHCs or RHCs for virtual check-ins via the AIR or PPS. The rate for G0071 will be set at the average of G2012, G2010, 99421, 99422 and 99423 Physician Fee Schedule rates which are updated annually. The current 2023 payment rate for G0071 is $23,72, the 2022 reimbursement rate was $23.88.
*The description for G2010 was excluded from the above coding section as store-and-forward technology is only permitted under certain circumstances in Alaska and Hawaii and not relevant to the intent of this document. However, this code is used for payment methodology purposes nationally.
When an FQHC practitioner gives a patient Virtual Communication Services, Medicare waives the FQHC face-to-face requirements and applies the coinsurance. For more information, refer to the Virtual Communication Services Frequently Asked Questions.
Billing Matrix
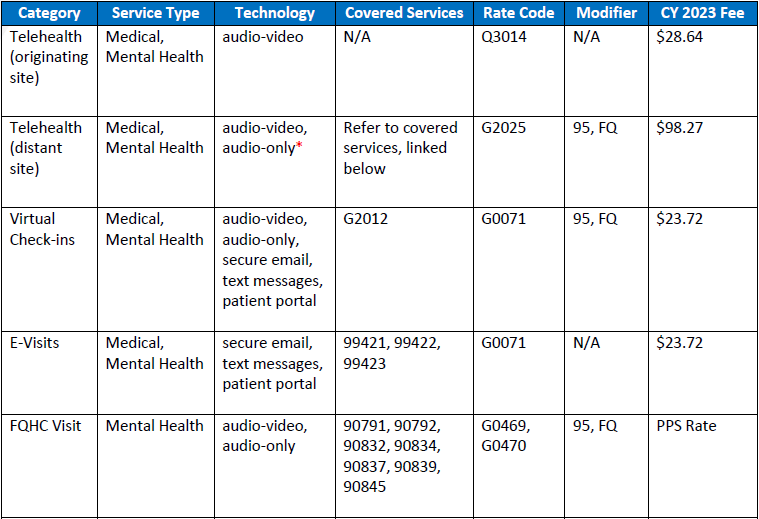
.
*Only certain telehealth services are allowed to be furnished via audio-only telecommunications systems. Please refer to the list of Medicare Covered Telehealth Services to identify when it’s appropriate to use audio-only.